The Hemp Connection
[
Search results for ovulation
]
Should you supplement? Chastetree berry (vitex) Part 1
The latest research regarding acupuncture and PCOS
Got PCOS and infertile? Watch out metformin, myoinositol is gaining notice!
Marijuana's effects on PCOS
Marijuana: Effects on the Endocrine Reproductive Systems
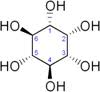
Mother Nature's way to increase your myoinositol levels
Inositol: Can it help you to ovulate?
Insulin sensitizers, d-chiro-inositol, and fertility
Chaste-tree Berries [Vitex agnus-castus]
Should you use flax during pregnancy?
We are making babies in Minnesota!
How do I know if I need a supplement?
Important Lab Tests for PCOS
What lab tests should I be getting in my PCOS assessment?
Induced abortions previous to IVF: an epidemiologic register-based study from Finland.
More about myoinositol
New Infertility Program Puts Mother Nature Back Into The Equation
New Infertility Program Puts Mother Nature (and the Clarendon Hotel) Into The Equation
Myoinositol, folate, and melatonin — the power fertility team
Magical thinking — don't let it undermine your PCOS success
Random for
run
:





![Chaste-tree Berries [Vitex agnus-castus]](https://blogger.googleusercontent.com/img/b/R29vZ2xl/AVvXsEia_cDxvXATK7NvDvO3BI3E68WG_FJpkCzGsuA5O5Ef_-EQFWoiuxEIN1ozE0NzKhjqRjhPCZK4R04X2OrHznPDLmJ0NJYvc2nFaQi0acQ_gSnVJl1KRPCGKSP6GTNQqtupcESngBPgYg/s1333/Vitex_agnus-castus_Montrose_Purple-6.jpg)








